Gender and Intersectionality Webinar – 10 January 2022
by Samina Huque, ARK Foundation
A webinar was arranged on ‘Gender and Intersectionality Planning” on 10th January 2022. The objective of the webinar was to provide guidance on using the gender and intersectionality framework (CHORUS’ Gender and Intersectionality Guide) to reflect on the data collection and to further shape the health systems intervention to be developed as part of the current CHORUS projects.

The webinar was led by Sushama Kanan, from ARK Foundation in Bangladesh, who provided a brief overview of the gender and intersectionality guidance and how to use it, looking at the Morgan et al. 2016 framework. She emphasized why gender and intersectionality are important for health systems research and how to ensure all dimensions of gender and the intersections with poverty and other social characteristics are incorporated into health systems research.
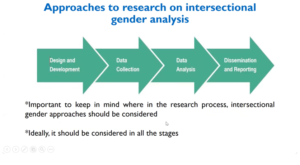
Abriti Arjyal from Herd International, Nepal, discussed the WHO TDR toolkit and provided an understanding of how it relates to the gender guidelines. She focused on examining the different steps that researchers need to consider while using the toolkit. She explained how gender power relations intersect with other social stratifiers, such as wealth, caste and disability, to create impact people’s lives. She highlighted the gender relations domains in terms of social stratifiers and infectious disease of poverty domain.
Dr. Joe Hicks from the University of Leeds then presented on how gender and intersectionality variables can be included during the secondary data analysis and designing the quantitative data collection (sampling tool) and analysis. In particular, he explained how we can look at the interactions between intersecting variables (gender, wealth, etc) rather than only exploring their additive effect.
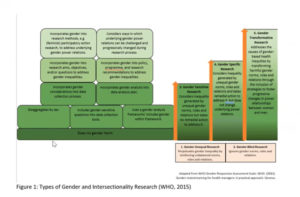
Dr Helen Elsey shared the WHO Gender Resource Assessment Scale (WHO, 2011. This can be found in the Gender and Intersectionality Guide). She pointed out the importance of talking about gender in research and considering gender and intersectionality during intervention design, and ensuring gender inequality is not perpetuated through research work. Under the WHO Scale, gender specific research takes action to remedy unequal norms and transformative research addresses root causes of inequality to transform social norms. While we are working for our project 1 research to be gender sensitive, we can use our intervention co-creating approach to take remedial or even transformative action to ensure no group is disadvantaged.
Breakout session topics:
Breakout rooms were divided as per CHORUS partner country teams. Each team consisted of qualitative and quantitative researchers, and discussed using the framework and guidelines for the CHORUS projects. Ideas were presented back to the group for wider discussion.

Ghana team:
Lauren Wallace fed back discussions from the Ghana Team. Discussion centered on the current stage of research; the process of data collection and adapting to interview guides. She highlighted that mapping is useful for future planning and to further identify stratifiers that can be of help. It is important to use different domains that Morgan identifies to make sure that the mapping covers them. The Ghana team is planning an initial capacity building exercise on the mapping procedure.
Nigeria team:
Chinyere Mbachu fed back discussions from the Nigeria team on how they would explore gender and intersectional analysis and constitute data while doing the quantitative data analysis, and find out the social stratifiers affecting the process. A challenge identified by the team is due to stakeholders not sensitized to gender differences and how it affects access to health care services. The team will address this by using the framework with different stakeholders for better outcomes. They will design dimensions that will sensitize them to gender differences and also finding stronger quantitative and qualitative baseline for feeding to stratification of stakeholders.
Bangladesh team:
The Bangladesh team from ARK Foundation have been in the field for the past month. Dr. Deepa Barua shared a number of issues that have arisen during this. In the open family health care context of Bangladesh, the males are at a disadvantage. The open family health care context mainly covers maternal and child health other than reproductive health, resulting in the male population being left out. The older population and transgender are also left out in the process. Dr. Barua also discussed the existence of hierarchy in the health sector; the decision maker is often the one with less experience which ultimately effects the quality of service provided to patients.
Dr Barua also raised who is included in the urban poor category in Bangladesh. Residency in a slum area doesn’t necessarily mean that you are classified as the urban poor in the city. For instance, in Dhaka City Corporation, urban poor have been segregated by the availability of something called the red card. There is this particular marking system. If you score 30 out of 100 then you are eligible for getting the red card, and you will receive medical services, medicines and operations for free. However, if your score is 31 out of 100, even if you are a poor slum dweller, you will not receive the red card and you will be excluded from services.
The Bangladesh team has incorporated different variables from the framework in their project design and are considering the impact of different variables on the health care service sector. The team are focused on creating interventions so that everyone gets quick services in line with the WHO recommendations.
 WHO 2020, Incorporating intersectional gender analysis into research on infectious diseases of poverty: a toolkit for health researchers (ISBN: 978-92-4-000845-8)
WHO 2020, Incorporating intersectional gender analysis into research on infectious diseases of poverty: a toolkit for health researchers (ISBN: 978-92-4-000845-8)
Key Recommendations from the Webinar:
- Understanding gender and intersectionality and why it is important in our health systems and how to incorporate it into health system research.
- We emphasized the Morgan framework and recommended all team members use this in the design and analysis of their data and in the intervention co-design process. This framework helps us consider gender as a power relation and driver of inequity in health systems and helps identify how power can be constituted and negotiated in the contexts where we work.
- We focused on the existence of hierarchy in the health sector
- We highlighted how gender sensitivity needs to be integral to our Project 1 research.
- We considered how to do gender and intersectionality analysis of secondary data and designing the quantitative data collection (sampling tool) and using this intersectional analysis within project 1. During developing data collection include questions that can help answering how gender and intersectionality affects the particular issues/outcomes that the research intends to explore.
- We suggest that those working on infectious diseases draw on the excellent TDR guidelines to ensure that all dimensions of gender and the intersections with poverty and other social characteristics are addressed.
The presentations and recording from the webinar are available:
Gender & Intersectionality webinar PowerPoints