
Blog: Working with Community Advisory Groups in Research: Lessons Learned from Bangladesh and Ghana
By Francis Poitier (University of Leeds), Lauren Wallace, Adanna Nwameme and Delali Kumapley (University of Ghana), Deepa Barua and Rumana Huque (ARK Foundation)
Urban October calls global attention to urban issues and the opportunities available for sustainable development. This year’s theme focuses on engaging youth to create a better urban future. Community engagement, including with youth, is a key component of CHORUS’s work. One way to engage youth and other groups is through community advisory groups.
CHORUS hosted a webinar on lessons learned from forming and engaging Community Advisory Groups (CAG) as part of projects in Bangladesh and Ghana. CAGs are a voluntary group of members of the community within the research setting, that advises researchers on the experiences, needs, and expectations of the affected community. They can form part of systematic patient and public involvement processes to ensure that affected communities are involved in all aspects of research, from planning, design, management, and implementation, to dissemination and translation of research findings into interventions. Working with CAGs form a component of participatory action research (PAR). PAR brings researchers and participants of research (e.g., communities, health workers, policymakers) together to collaboratively reflect, plan and act in order to address collective problems.
CAGs were important to understanding the community perspective, engaging communities in all aspects of the research projects and ensuring that research findings were valid. Engagement with CAGs was also important as communities would be part of intervention implementation.
By exploring examples shared by researchers conducting work in urban health in Bangladesh and Ghana, this post summarises the webinar discussions by focusing on three key areas: (i) why and how to form CAGs; (ii) how to engage CAGs in implementation research; and (iii) challenges, mitigation and lessons learned.
Why and how to form Community Advisory Groups
CAGs can enrich and empower communities through the research process. For communities, it can amplify the public voice in decision-making, bring individuals together who share common experiences, and provide a platform for further community building. It can help communities learn about research and develop skills such as problem solving, creative thinking, and critical thinking.
For researchers, community involvement throughout the research cycle can help to identify and prioritise research problems, support innovative methodologies and design, and ensure that research has an impact by reaching communities and intended stakeholders.
In Bangladesh, Professor Rumana Huque and Dr. Deepa Barua of ARK Foundation shared the experiences of forming two CAGs related to their research on “Strengthening the urban primary health care system to manage essential Non-Communicable Disease care among the urban poor”. When forming the CAGs, gender, NCD status, education level, employment status, and power dynamics were important to consider. It was advantageous to form two separate CAGs to ensure a balance of exploring demand-side factors (from the community) and supply-side factors (from health workers). Both groups would also be involved in any interventions developed and implemented.

- One CAG was comprised of urban dwellers (slum dwellers and people from lower income backgrounds) to better understand perceptions of the healthcare system, health facilities and health-seeking behaviour related to non-communicable diseases (NCDs) and to learn about community expectations of and suggestions for health services in the local community. Through this CAG, urban dwellers shared challenges in making lifestyle changes due to schedules, stigma and unclear guidance, how it was difficult to continue NCD medications due to the high costs, and being dependent on pharmacies rather than healthcare centres.
- The other CAG was comprised of healthcare workers from different types of urban primary healthcare facilities such as medical assistants (Sub-Assistant Community Medical Officers from Government Outdoor Dispensaries and paramedics from NGO Clinics) and pharmacists. This was to understand better how these facilities operate and the challenges faced, to learn about the types of NCD patients and their care pathways, and to gather suggestions for strengthening health services. Healthcare workers shared that they faced several challenges regarding poor health infrastructure, personal safety, job security due to sudden job transfers, and the lack of adequate support in their roles. Due to the range of services offered, it also meant that they could not specifically focus on NCDs. Healthcare workers who worked in NGO clinics also faced additional challenges due to not having sufficient supply of NCD medications, not being supported by the Ministry of Health and Family Welfare. Additionally, the requirement of having to generate revenue, despite being supported by funds from the Ministry of Local Government, Rural Development and Cooperatives, and the Asian Development Bank, has led them to deliver services with a focus on reproductive, maternal, newborn and child health.
Similarly, in Ghana, Dr. Lauren Wallace of the University of Ghana shared experiences of forming two separate CAGs in each of the municipalities where research on “Improving the functioning and scope of the Community Based Health Planning and Services Initiative in urban settings” was taking place.
- Each CAG consisted of a diverse range of relevant stakeholders. It included members of the local government, community associations representing different cadres of workers, religious and traditional leaders, community health committee members, community members from vulnerable groups, and health workers. There was a balance of voices from community members and health workers. The makeup of the CAG was part of the result of a stakeholder mapping and analysis to identify groups and individuals important to the research and to ensure representation of differing perspectives, interests, values, and political affiliations. Having local government leaders and other opinion leaders involved from the onset was advantageous because these members may be positioned to support resource mobilisation.
How to engage CAGs in research
While CAGs can be engaged in all aspects of research, it is important to be clear about what is expected of members. This includes having a common understanding of the group’s focus and how frequently they can expect to be engaged.
In both countries, Terms of Reference were developed which clearly identified roles and responsibilities, the focus of the CAGs, and expectations of the group, including their involvement in intervention implementation. It also outlined how the research teams would regularly share updates with the CAG and engage them through troubleshooting, areas of concern, research findings and more.
CAGs were engaged from the beginning of the research process. For example, in the needs assessment phase, they shared their thoughts and insights while in the co-creation phase they helped with the development of potential interventions. It is hoped that this frequent engagement will help with the sustainability of interventions developed.
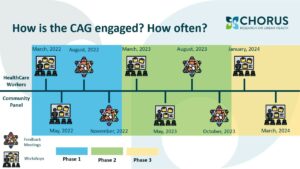
In Bangladesh, the groups were engaged through workshops and feedback meetings in each important phase of the research (approximately five times for each CAG between 2022 and 2024)
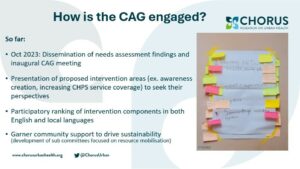
In Ghana, there were also meetings and workshops (see Figure 2). One workshop included a participatory ranking approach, where CAG members first individually ranked intervention areas and shared ideas, before the research team developed a finalised comprehensive group ranking and agreed on it with the CAG. The final intervention was presented and possible implementation timeframes were agreed upon in another workshop with the CAG. The members also provided feedback on the awareness creation materials and messages including where the materials should be displayed in the various communities and in what languages the messages should be translated for maximum impact to be achieved. The workshops were held in English and local languages.
Challenges, mitigation and lessons learned when using CAGs in research on urban health
The teams in Bangladesh and Ghana identified some common challenges and mitigation techniques when engaging CAGs, summarised in the image below.
